

“You Took It, You Own It”
Is a general dentist required to look at all the data in a CBCT scan?
Yes, in the United States and Canada, a general dentist who orders or interprets a CBCT scan is expected to evaluate the entire imaged volume, not just the region of immediate dental interest (for example an implant site).
That expectation comes is supported by multiple professional, legal, and risk-management principles:
The practitioner who orders the scan assumes responsibility for findings visible within the captured field of view (FOV).
Incidental findings outside the teeth are common in CBCT images.
Failure to recognize or appropriately refer significant abnormalities can create malpractice exposure.
Professional organizations including the American Academy of Oral and Maxillofacial Radiology and the American Dental Association have emphasized that the entire dataset should be reviewed, either by the treating dentist if competent to do so, or by a qualified radiologist.
Examples of non-dental findings that may appear in a CBCT volume include:
Carotid artery calcifications – “plaques”
Medial arterial calcifications (MAC) related to diabetes
Sinus disease
Airway abnormalities
Cervical spine pathology
TMJ abnormalities
Cysts or tumors
Enlarged tonsils and adenoids
The key distinction is competence:
A general dentist is not expected to have the same expertise as an oral and maxillofacial radiologist.
However, they are expected to recognize when interpretation exceeds their training and obtain an appropriate radiologic consultation.
When you don’t know what it is you’ve found, refer!
In practical terms, many dentists reduce liability by using smaller fields of view when clinically appropriate. However some incidental and important findings may still be present.

Image 1: Not a "diffuse, sclerotic plaque", but a linear calcification along the wall of the internal carotid artery.
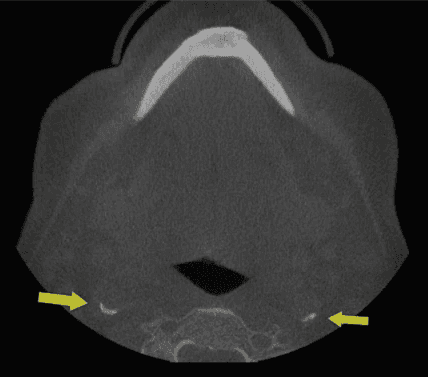
Image 2: Curvilinear, almost circular calcification in/around the wall of the right internal carotid artery.
Both images suggest suggest medial arterial calcification seen in Type 2 Diabetes Mellitus.
Having all large-volume CBCT scans formally interpreted by an oral and maxillofacial
radiologist.
Using structured reporting workflows and AI triage tools to help identify abnormalities,
while still maintaining clinician oversight.
Courts and dental boards typically focus less on “Did you personally diagnose everything?” and more on:
Was the scan reasonably reviewed?
Were obvious abnormalities ignored?
Was referral obtained when appropriate?
Was the patient informed of significant findings?
This is one reason comprehensive reporting systems and radiology overreads have become increasingly important in CBCT practice.
Reference
Friedland B and Miles DA. Liabilities and Risks of using Cone Beam Computed Tomography. Dent Clin N Am 58: (2014) 671–685.
Dayo AF, Miles DA and Hamann BR: Detection of medial arterial calcification on CBCT images of a patient with undiagnosed type 2 diabetes mellitus: a case report. General Dentistry 69(5): 57-61, 2021..
related news
Latest industry trends and
expert
insights from our team
Keep up with our newest projects, market trends, and expert insights
